

Your Medical Record Has a Chat Box
Plus: Patient portals get conversational, health search trust stays messy, and UpDoc shows where AI care needs hard rails.


Your daily signal on AI and CX — minus the hype.
DCX Stat of the day: Hartford HealthCare’s PatientGPT beta has logged more than 8,300 conversations with about 6,000 unique patients. CT Insider
In this issue:
→ Patient portals get an AI front door
→ Health answers need identity and consent
→ Search trust stays very messy
→ UpDoc puts boundaries around AI care
→ Care handoffs need visible ownership
🔍 DEEP DIVE
The Portal Starts Talking Back

Hartford HealthCare recently rolled out PatientGPT, a chatbot inside its patient portal that can explain lab results, answer questions using a patient’s medical record, help with scheduling, check drug interactions, and summarize questions a patient may want to send to a clinician.
That is a very different thing from typing symptoms into a public chatbot at midnight.
The useful part is context. The risky part is also context. Once AI can read from a patient’s actual record, the experience is no longer generic health education. It is authenticated, personal, and dangerously easy to over-trust.
Hartford’s model includes patient permission, limits on prescribing or recommending specific treatment, and escalation paths. Good. That is the floor, not the finish line.
The CX question is simple: when a patient asks an AI to explain something scary, confusing, or expensive, who owns the answer the patient acts on?
Bottom Line: Health AI gets more useful when it knows the patient, and more dangerous when the organization has not defined consent, escalation, clinical boundaries, and explanation in plain language.
📬 Copy-Paste Take
Before we put AI inside a patient record, we need a written boundary map: what it can explain, what it cannot recommend, when it must escalate, what gets written back to the record, and how the patient knows a human clinician has taken over.
🧭 OPERATOR PLAYBOOK
Put the Boundary Where the Customer Can See It
Pick one journey where AI uses authenticated customer data to explain, recommend, summarize, triage, or trigger a next step.
Health portal. Banking app. Insurance claim. Benefits decision. Account recovery. Financial advice. Subscription change.
Audit every authenticated AI interaction for four things:
Permission: Did the customer knowingly allow this data to be used here?
Boundary: What can the AI explain, suggest, or do?
Escalation: What phrase, risk, or uncertainty sends the case to a person?
Record: What answer, action, or handoff is logged for later review?
Then test whether a normal customer can see the line.
Not the policy line. The experience line.
Can they tell when the AI is explaining information, when it is suggesting a next step, and when a qualified human has taken responsibility?
Ask your team: Where could AI sound helpful while quietly making the customer more dependent on an answer no one owns?
Signal: Authenticated AI needs visible boundaries more than better prompts.
📊 MARKET REALITY CHECK
The Trust Gap Is Already in the Waiting Room
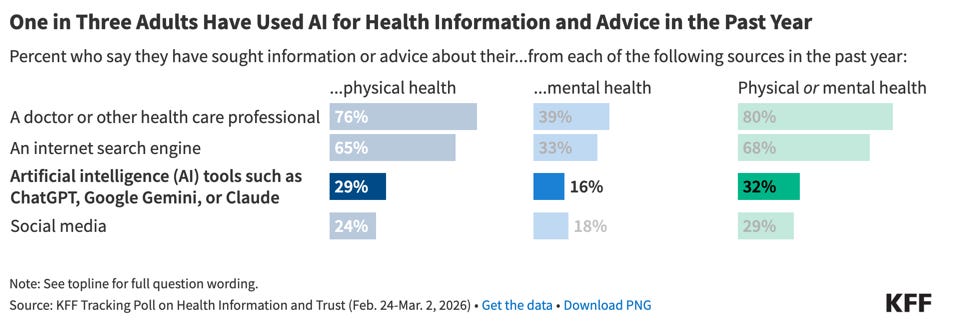
KFF’s latest health-information trust polling found that 1 in 3 adults are turning to AI chatbots for health information, roughly equal to the share using social media for health information.
That number does not prove people want AI to replace a clinician. It proves patients are already pulling AI into the journey before the healthcare system is ready to manage the handoff.
This is where the operating work gets uncomfortable. Patients may use a public chatbot, a search result, a portal assistant, a nurse line, and a clinician message inside the same decision. Each touchpoint can sound authoritative. Each one can send the patient in a different direction.
The lesson for healthcare leaders is not “add a chatbot.” It is: make the trusted path easier to find than the random path.
Why it matters: If patients are already using AI for health answers, the experience has to show which answers are general, which are record-specific, and which require clinical review before the patient acts.
Helpful answer + unclear authority = patient risk
🧰 TOOL WORTH KNOWING
UpDoc
What it does: UpDoc positions itself as a clinician-led AI care platform for chronic disease management, preventive care, intake, follow-up, and patient check-ins.
CX use case: Helping care teams stay connected to patients between visits, especially when the work involves reminders, readings, adherence, follow-up questions, and clinician-defined treatment boundaries.
Worth watching because: Between-visit care is where healthcare CX usually gets mushy. The patient is at home, the clinician is busy, the portal is passive, and the next small problem becomes tomorrow’s expensive escalation. UpDoc points to a more active model: AI can nudge, collect, route, and support the patient, but only if the care plan and escalation rule are not vibes in a white coat.
Bottom line: AI follow-up is useful when it extends the clinician’s plan, not when it freelances around it.
The DCX AI Today - AI Tool Directory - If you lead a CX team and want a curated shortlist of tools worth evaluating, this is your starting point.
✅ YOUR MOVE
AI is moving from public answers into authenticated customer journeys.
That makes consent, authority, escalation, and handoff design part of the experience.
Run this test on one high-trust journey this week:
When AI explains something personal, can the customer tell where the system’s authority begins and ends?
Check four moments:
What the AI can safely explain.
What it can never decide.
When it must route to a person.
What the customer sees when ownership changes hands.
If the boundary is only visible in the policy deck, it is not visible enough for the customer.
If AI uses the customer’s record, the boundary has to be visible to the customer.
Until tomorrow,
👥 Share This Issue
Think of one person who’s wrestling with AI in CX right now
and forward this to them.
I’m obsessed with Wispr Flow Pro! Get a Free Month on me.

If someone forwarded this to you, they thought you needed to see it before your next AI planning meeting. Get your own copy.